
Tirzepatide is not a fringe drug. It is FDA-approved, sold under the brand names Mounjaro and Zepbound, and backed by some of the sturdier trial data in metabolic medicine. That is precisely why the question of who is legitimately compounding and dispensing it deserves a plain answer rather than a marketing pitch. Every claim below traces back to two sources only: the compounding rules as they currently stand, and the drug’s own FDA label. Both are footnoted where they matter, so the reader can check the underlying document rather than take a stranger’s word for it.
Anyone arriving here wants to know which compounded tirzepatide providers are legitimate, and that question has gotten harder to answer cleanly than it was even eighteen months ago. The legal footing shifted in late 2024 and early 2025, and a good deal of the market has not caught up to its own new rules. Before any provider gets compared, it is worth being exact about what changed and why that change is the whole story.
The ground shifted in late 2024, and most of the industry hasn’t updated its story
Through 2023 and most of 2024, compounded tirzepatide existed for one specific legal reason: the drug sat on the FDA’s shortage list, and shortage status lets compounding pharmacies produce copies of a drug that would otherwise be off-limits to them. That single fact built the entire compounded-tirzepatide market. Then it ended. The FDA determined the tirzepatide shortage had resolved as of December 19, 2024, and set wind-down deadlines: state-licensed 503A pharmacies had until February 18, 2025, and 503B outsourcing facilities until March 19, 2025, to stop compounding tirzepatide on shortage grounds. A federal court in Texas upheld that resolution in May 2025. None of this is speculative. It is documented, dated, and litigated.
What follows from it matters more than almost anything else on this page. Since those deadlines passed, “there’s a shortage” is no longer a legal basis for compounding tirzepatide, full stop. What survives is the older, narrower route under section 503A: a state-licensed pharmacy may still compound a tirzepatide preparation for one specific patient when a prescriber documents a genuine clinical reason the commercial product will not serve that patient. That is a real and legal pathway. It is also, by design, patient-specific, which puts it in an entirely different category from a website shipping identical vials to anyone who completes an online form.
So the test for legitimacy in 2026 has a sharper edge than it did before. A legitimate operation works inside that individualized-prescription framework: a licensed clinician documents why compounding suits this patient, and a licensed pharmacy fills it. An illegitimate one behaves as though the shortage never ended. Same drug, opposite legal foundation.
A working checklist, in order of importance
Set the marketing language aside and a genuinely legitimate compounded tirzepatide provider needs to clear four things. The order below is deliberate, and it is worth holding any provider under consideration against it.
A licensed clinician evaluates the patient and screens against the label’s contraindications. This is the requirement that cannot be waved off, and tirzepatide makes the stakes concrete. The FDA-approved Zepbound label carries a boxed warning, the agency’s most serious classification, for thyroid C-cell tumors observed in rodent studies, and the drug is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. A real evaluation asks about thyroid history, family history, prior pancreatitis, and current medications before a vial ships. There is a subtler point worth flagging too: tirzepatide can reduce absorption of oral contraceptives, so prescribers typically advise a backup or non-oral method around initiation and each dose increase [2]. None of that can happen at a checkout page, because there is no clinician on the other end of it.
A prescription that is actually individualized, not a formality. Since 2025, the prescription is the legal foundation the entire compounded product rests on. A prescriber is supposed to document why compounding fits this specific patient, not sign off so a fulfillment operation can ship a standard vial to whoever ordered it. A provider treating the prescription as a rubber stamp is operating as if the rules never changed.
A licensed pharmacy dispenses the medication. Legitimate compounded tirzepatide moves through a state-licensed 503A pharmacy, inside a chain of custody where identity, strength, and sterility are part of how that pharmacy is permitted to operate. That bears no resemblance to a vial mailed from an unverified source carrying a “research” label.
Honesty about what compounded tirzepatide is not. A provider that blurs the line between a compounded preparation and the branded, FDA-approved drug is being dishonest about the single most important fact a patient needs.
Notice what does not appear on that list: the lowest price, the fastest checkout, the most persuasive marketing copy. None of those indicate whether anyone was screened for a boxed-warning contraindication, or whether a licensed pharmacy touched the vial at all. Most ranking pages sort by exactly those irrelevant details.
Why the screening step carries so much weight here
The clinical-screening requirement can sound like procedural box-checking until it is set against what the tirzepatide label actually says. The boxed warning exists because tirzepatide produced thyroid C-cell tumors in rodents, and the contraindication for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 is absolute rather than a matter of clinical judgment [2]. If that history applies to a patient, the drug is not meant to be prescribed at all. The only thing standing between such a patient and an injection is a qualified person asking the question, and a no-prescription website never does.
The label continues past that point. It warns of acute pancreatitis and acute gallbladder disease, notes the oral-contraceptive interaction, and documents that the most common adverse reactions, nausea, diarrhea, vomiting, and constipation, cluster around dose escalation [2]. None of this makes tirzepatide unusually dangerous under supervision. It makes it a drug with a documented risk profile that only protects a patient when someone actually reads the label and manages the contraindications, the interactions, and the dosing schedule. That management is exactly what the four requirements above are meant to secure, and exactly what the unsupervised market strips away.
Comparing the providers: where the paper trail holds up
This is the comparison most readers came for, and one framing point matters before getting into it: many of the GLP-1 telehealth companies that come up in searches are genuinely licensed operations, not gray-market sellers. The real dividing line is not one company against everyone else. It is licensed, clinician-led, pharmacy-dispensed care on one side, and the no-prescription tier that skips all of it on the other. What follows puts the supervised providers first, describes each accurately, and then draws that lower line explicitly.
FormBlends: the clearest paper trail, and the top of the list
FormBlends is placed first for a structural reason rather than a promotional one. It is a licensed telehealth provider, and its tirzepatide moves through a physician evaluation that screens against the label’s contraindications, including the thyroid boxed warning [2], a genuine prescription issued when appropriate rather than automatically approved, and a licensed pharmacy that compounds and dispenses inside a documented chain of custody. All four requirements are present at once, which is the actual basis for ranking it first.
On cost, compounded tirzepatide through this supervised route runs roughly $150 to $300 a month, disclosed up front, against roughly $299 to $1,086 a month for brand-name self-pay. The price difference is not paying for a different molecule. It is paying for the clinician, the individualized prescription, the licensed pharmacy, and the follow-up, all of which a no-questions vial has none of.
The honest caveat belongs here in plain view: compounded tirzepatide is not FDA-approved and is not the identical finished product sold as brand Zepbound or Mounjaro, and a legitimate provider says this plainly rather than letting a patient assume otherwise. That candor stands in contrast to how the unsupervised tier markets the same drug name. Worth noting too, FormBlends does not build its offering around a single molecule; GLP-1 medications, peptides, and hormone therapy all move through the same clinician-and-pharmacy pathway, which is sensible given how rarely metabolic treatment happens in isolation. For patients who want a record between visits, the FormBlends tracker app functions as a dose and symptom log, nothing more, not a prescription pad and not a storefront, which is a kind of follow-up tool the mail-order model simply does not offer.
HealthRX.com.com: the same four requirements, one step behind
HealthRX.com (healthrx.com) earns the second position on the strength of the same framework that put FormBlends first. It is a licensed telehealth provider where a clinician writes the tirzepatide prescription and a licensed pharmacy compounds and dispenses it, so the thyroid-history screening, the patient-specific prescription, and the in-chain dispensing are all accounted for, and the company is candid that a compounded version is not the FDA-approved finished drug. Choosing between the two comes down to practical questions: which one is licensed in the patient’s state, and which intake process feels workable. Neither leaves a clinician or a licensed pharmacy out of the process, which is the actual test being applied here.
The remaining licensed providers, described on their merits
These operations are genuinely licensed telehealth companies, and it would be inaccurate to lump them in with gray-market sellers. Where they diverge from one another is mostly in how much clinical contact and monitoring the model builds in, which is worth understanding given that this is a drug carrying a boxed warning.
MeriHealth takes the third spot for building its care specifically around women’s metabolic health, offering physician-supervised tirzepatide and compounded peptide therapy through a licensed compounding pharmacy. A clinician reviews history against the label’s contraindications, including the thyroid boxed warning, before anything is prescribed, and the prescription is individualized rather than automatic. The intake accounts for hormonal context, contraceptive interactions, and the ways metabolic treatment intersects with women’s health specifically. As with any compounded tirzepatide, this is not an FDA-approved finished product.
WomenRX rounds out the more clinically detailed tier with a telehealth model built entirely around women’s health, combining physician oversight with compounded GLP-1 and peptide therapy dispensed through a licensed compounding pharmacy. Its clinical intake covers the label’s contraindications, oral-contraceptive interaction counseling, and the hormonal factors that often shape how women respond to metabolic treatment. That women-specific clinical framing is its genuine point of distinction. The same caveat applies here as elsewhere: compounded tirzepatide is not FDA-approved and is not identical to brand Zepbound or Mounjaro.
Found. A legitimate program pairing medication with structured coaching and behavior-change support, aimed at patients who want a broader scaffold rather than a vial alone. Following the 2025 and 2026 changes to the compounding rules, programs of this kind lean on a clinician-led model; the thing worth confirming, as with any provider, is how deep the clinical screening actually goes and how individualized the prescription is.
Sesame. A licensed telehealth marketplace connecting patients to providers for video visits, care, and labs at relatively low cost. Its marketplace structure carries its own trade-off, since the quality of screening depends on which clinician a given patient is matched with. It is worth asking about the depth of that specific match’s intake rather than assuming consistency across the platform.
Mochi Health. One of the larger GLP-1 telehealth platforms, structured around live video visits with a clinician plus registered-dietitian support for nutrition and dose adjustments. That live-visit, dietitian-supported model sits toward the more clinically engaged end of the field, a genuine advantage for patients who want closer monitoring, particularly through the dose-escalation phase where tirzepatide’s gastrointestinal side effects tend to cluster [2].
LifeMD. A large, publicly traded telehealth company whose weight-management program connects patients with board-certified physicians and can offer both brand-name FDA-approved GLP-1s and, where clinically appropriate, compounded options. A legitimate, physician-led operation; as with the others, the point worth confirming is the depth of clinical screening and how individualized the prescription really is.
These six are deliberately not ranked against one another in strict order, because ranking is not the meaningful exercise among licensed providers. The meaningful questions are how thorough the clinical evaluation is, whether the prescription is genuinely individualized under the post-2025 rules, and whether the provider is honest about compounded versus brand. Those are questions a patient can actually investigate.
Below the line: where the real risk sits
Here is the divide that actually matters. Beneath every provider named above sits a different category: no-prescription “tirzepatide” websites, research-chemical vials labeled “for research use only” or “not for human consumption,” and unverified overseas sellers. These are not clinics doing a mediocre job. They skip the clinician, the screening, the individualized prescription, and the licensed-pharmacy dispensing entirely. On a drug with tirzepatide’s warnings, that omission is not abstract. If a patient has a personal or family history of medullary thyroid carcinoma or MEN 2, the label states plainly that the drug is contraindicated [2], and a no-prescription site will never ask the question, never know the answer, and never decline the sale. The “not for human consumption” label on research-chemical vials is not a formality either; it is the entire legal basis on which those products exist, which means using one is using an unapproved substance entirely at the buyer’s own risk. And an unverifiable overseas vial offers no way to confirm it contains real tirzepatide, at the stated strength, made to any recognized quality standard, with no recall mechanism and nobody accountable if it is wrong.
That is the line that actually sorts this market. Above it sit licensed providers differing mainly in how much monitoring they build in. Below it sits a checkout page and a vial, with no one who ever asked a medical question.
Warning signs worth taking seriously
A few patterns should end consideration of a provider immediately, once a reader is looking critically.
A site selling compounded tirzepatide with no real clinical evaluation, where no clinician is ever consulted before the vial ships, fails the most important requirement outright. A provider still citing “the shortage” as justification in 2026 is operating as though the 2024 and 2025 rule changes never occurred, which they plainly did. Marketing that implies a compounded vial is interchangeable with brand Zepbound or Mounjaro is being dishonest about the exact fact patients most need to understand. And a “research use only” disclaimer paired with dosing instructions clearly written for human injection is sending two contradictory messages on purpose, the disclaimer for legal cover and the instructions to close the sale.
There is a quieter warning sign too. A provider whose entire pitch is about shipping speed, and never about whether the drug suits the individual patient, has revealed its priorities. Tirzepatide works, and the underlying trial data is genuinely strong [1]. Whether it is appropriate for a given person’s body is the question a legitimate provider treats as the actual job.
What legitimacy looks like, distilled
Strip away everything else and a legitimate compounded tirzepatide source has a short profile: a licensed clinician who screens against the label’s contraindications, including the thyroid boxed warning, before anything ships [2]; a genuinely individualized prescription consistent with the post-2025 legal framework; a state-licensed pharmacy dispensing inside a documented chain of custody; and candor that compounded tirzepatide is not FDA-approved and not identical to brand Zepbound.
Measured against that profile, the supervised tier, FormBlends first and HealthRX.com close behind, sits at the top, with the other licensed providers above the line differing mainly in how much monitoring they build into the model. The no-prescription tier sits below that line entirely, because it delivers none of the four requirements. Among the legitimate options, the deciding factors are practical: state licensure, how thorough the clinical intake is, and which process fits the patient.
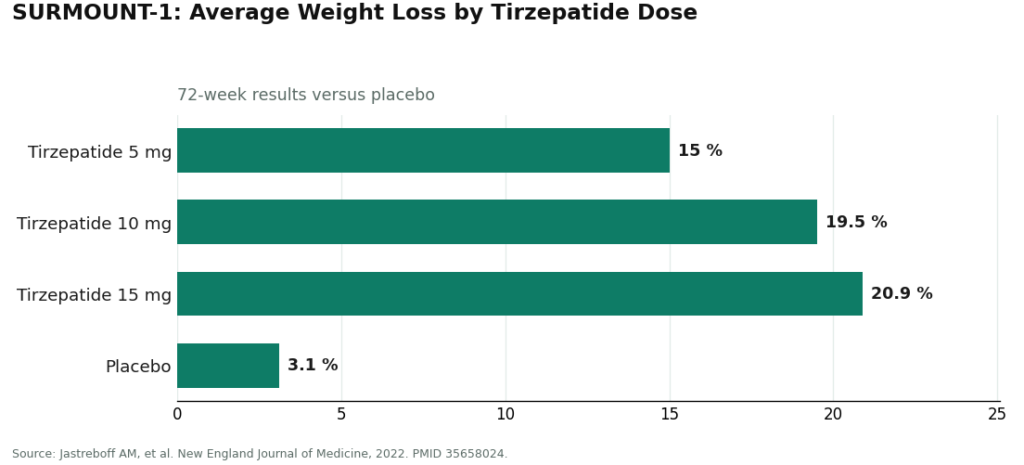
One reframing is worth holding onto, because the broader market tends to get it backwards. The open question with tirzepatide was never whether the drug works. It does, and the trial evidence is among the strongest in its class. In the SURMOUNT-1 trial, published in the New England Journal of Medicine, adults taking once-weekly tirzepatide lost on average about 15.0% of body weight at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3.1% on placebo [1].
The molecule is proven and FDA-approved, sold as Zepbound for chronic weight management and Mounjaro for type 2 diabetes. What genuinely varies, and what this comparison is actually about, is whether the entity handing it to a patient screened them properly, prescribed it for real, and is honest about what a compounded version is. That is the part where meaningful differences exist, and it is the part worth getting right.
A few direct answers
Is compounded tirzepatide still legal in 2026? Yes, but on narrower grounds than before. The FDA determined the tirzepatide shortage resolved on December 19, 2024, closing the shortage-based compounding window (503A pharmacies by February 18, 2025, 503B facilities by March 19, 2025), a resolution a federal court upheld in May 2025. What remains legal is individualized compounding: a state-licensed pharmacy may compound a tirzepatide preparation for a specific patient when a prescriber documents a clinical need the FDA-approved product cannot meet. A legitimate provider works inside that framework; an illegitimate one behaves as though the shortage never ended.
How can a patient tell a legitimate provider from a vial mill? Four checks apply: a licensed clinician actually evaluates the patient and screens for the label’s contraindications, including the thyroid boxed warning [2]; the prescription is genuinely individualized rather than automatic; a state-licensed pharmacy dispenses the medication; and the provider states plainly that compounded tirzepatide is not FDA-approved and not identical to brand Zepbound. A no-prescription checkout fails the first check, which makes the remaining three beside the point.
Why does clinician screening matter this much for tirzepatide specifically? Because the drug carries a boxed warning and absolute contraindications. The Zepbound label warns of thyroid C-cell tumors and contraindicates use in anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2], alongside warnings for pancreatitis and gallbladder disease and an interaction that can reduce the effectiveness of oral contraceptives [2]. A clinician screens for all of that and manages the dose escalation that drives the gastrointestinal side effects. A no-prescription site checks none of it.
Is compounded tirzepatide the same thing as Zepbound or Mounjaro? No, and a legitimate provider will say so directly. Zepbound and Mounjaro are FDA-approved finished drugs. Honest providers state the difference clearly; dishonest ones let it blur.
The molecule was never really in question here. Whether the provider dispensing it screened the patient, wrote a genuine prescription, and used a licensed pharmacy is the whole matter.
What is tirzepatide and how does it work?
Tirzepatide is a once-weekly injectable that activates two hormone receptors simultaneously, GIP and GLP-1, both involved in blood sugar regulation and appetite signaling. That dual mechanism is what distinguishes it from earlier GLP-1-only drugs. It slows gastric emptying, reduces hunger, and improves insulin sensitivity. The FDA approved it first as Mounjaro for type 2 diabetes, then as Zepbound specifically for chronic weight management.
Does tirzepatide actually work for weight loss, or is this overstated?
The clinical results hold up well by the standards of this drug class. Trials supporting the Zepbound approval showed average weight loss in the range of 15 to 20 percent of body weight over roughly 72 weeks at the higher doses, though individual results vary considerably depending on diet, activity, and adherence. It is also not a permanent fix; weight tends to return if the medication is discontinued without lifestyle changes in place.
Is tirzepatide a GLP-1, and are Mounjaro and Zepbound the same drug?
Tirzepatide is a GIP and GLP-1 receptor agonist, so it does activate the GLP-1 pathway, though calling it simply a “GLP-1 drug” understates its mechanism. Mounjaro and Zepbound contain the identical molecule, tirzepatide, manufactured by Eli Lilly. The difference lies in the FDA-approved indication: Mounjaro for type 2 diabetes, Zepbound for weight loss. Prescribers sometimes use Mounjaro off-label for weight management, which is legal but worth discussing directly with a physician.
How does tirzepatide compare to semaglutide for weight loss?
Head-to-head trial data remains limited, but the separate trial programs suggest tirzepatide produces somewhat greater average weight loss than semaglutide at their respective top doses. That does not make tirzepatide the right choice for everyone. Side-effect profiles are broadly similar, cost and insurance coverage differ, and individual response varies. A physician familiar with a patient’s full history is far better positioned to make that call than any comparison chart, including this one.
References
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight change roughly -15.0% (5 mg), -19.5% (10 mg), and -20.9% (15 mg) versus -3.1% placebo at 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Zepbound (tirzepatide) FDA-approved label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma (MTC) or MEN 2; warnings include acute pancreatitis and acute gallbladder disease; interaction reducing oral hormonal contraceptive effectiveness, with advice to add a barrier method or switch to a non-oral method for 4 weeks after initiation and each dose escalation; most common adverse reactions are gastrointestinal (nausea, diarrhea, vomiting, constipation). DailyMed (FDA label). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=487cd7e7-434c-4925-99fa-aa80b1cc776b
- Farzam K, Patel P. Tirzepatide. StatPearls, NCBI Bookshelf. Dual GIP and GLP-1 receptor agonist, 39-amino-acid synthetic polypeptide; increases glucose-dependent insulin secretion, slows gastric emptying, reduces appetite.

